Definition of "Bowel obstruction"
Last modified: about 1 year
Bowel is just another word for intestine. So it's just anything that's obstructing the intestine from what it normally does, which is carry feces.
Constipation happens, because feces can't get through. The tummy can be enlarged, because feces is building up. If feces keeps building out, it can come out the mouth, as fecal vomiting.
You can start with bloods. You can also take images, including an x-ray of the tummy. Because x-rays aren't that good to see soft tissue, you can use contrast to outline the inside of the GI tract. Or you can use ultrasound or CT, which is better for soft tissue. You can also put a camera down the throat, to look inside, and pinch a bit of the thing that's causing the blockage.
If the patient isn't eating, you can put a tube down their nose and feed them that way. If they're in pain or vomiting, you can also fix that. You can do open surgery. Or you may be able to use a stent to relieve any obstruction that you find.
All the vomiting can cause a patient to become dehydrated, and affect electrolytes. The expanding mass in the tummy, can also put pressure on the diaphragm, even affecting the patient's breathing. A blockage can also cause the tummy system to blow up, or put pressure against it's blood supply, and kill parts of it.
Bowel/intestinal obstruction is mechanical/functional obstruction of the intestine, preventing normal transit of feces.
SBO is shorthand for Small bowel obstruction.
Patient information
What is bowel obstruction?Bowel is just another word for intestine. So it's just anything that's obstructing the intestine from what it normally does, which is carry feces.
Sx
- Sx depends on the level of obstruction
- Abdominal pain, which tends to be:
- In small bowel obstruction:
- Colicky (cramping and intermittent) in nature, w/ spasms lasting a few minutes
- Pain tends to be central and mid-abdominal
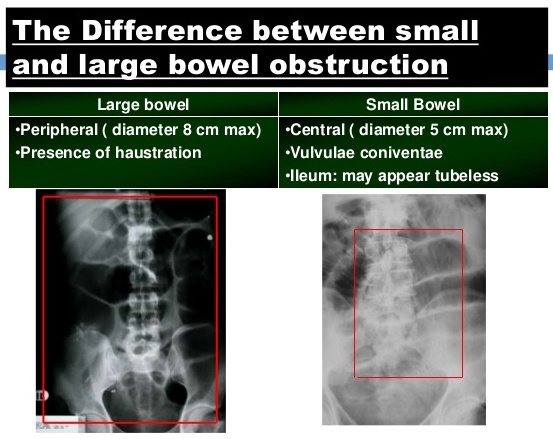
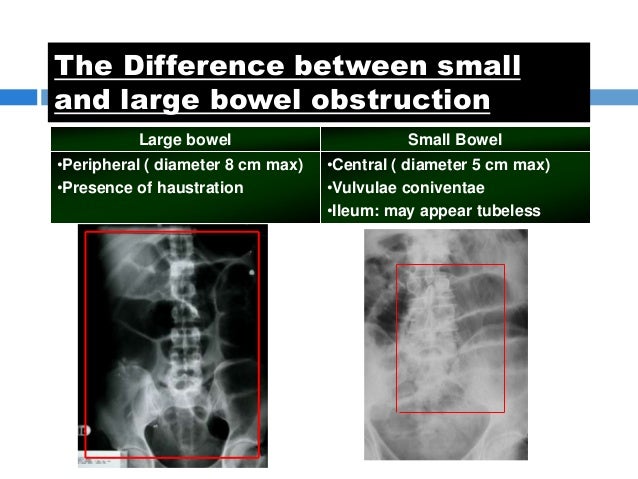
- In large bowel obstruction:
- Pain felt lower in the abdomen, w/ spasms lasting longer
- Constipation occurs earlier
- Proximal obstruction of the large bowel may present as small bowel obstruction
- In small bowel obstruction:
- Swollen abdomen
- Abdominal distension
- Vomiting, including fecal vomiting
- In small bowel obstruction, vomiting may occur before constipation
- In large bowel obstruction, vomiting may be less prominent
- Constipation, absence of normal stool/flatus
- Increased bowel sounds
Patient information
What is it like if you get an intestinal obstruction?Constipation happens, because feces can't get through. The tummy can be enlarged, because feces is building up. If feces keeps building out, it can come out the mouth, as fecal vomiting.
Is there any tummy pain?
Tummy pain, is seen in both obstruction of the small and large intestine. But whereas the pain is more central and colicky in the small intestine... when it gets to the later large intestine, the pain is lower, and the spasms last longer.
Pathophysiology
- Can occur at any level distal to the duodenum (of the small intestine)
Cause
- Small intestine obstruction, including:
- Adhesions from previous abdominal surgery, most commonly
- Pseudoobstruction
- hernias containing bowel
- Crohn's disease, causing adhesions or inflammatory strictures
- Neoplasms, benign or malignant
- Intussusception in children
- Volvulus
- Superior mesenteric artery syndrome, a compression of the duodenum by the superior mesenteric artery and abdominal aorta
- Ischemic strictures
- Foreign bodies, e.g. gallstones in gallstone ileus, swallowed objects
- Intestinal atresia
- Large intestine obstruction, including:
- Neoplasms
- Diverticulitis/diverticulosis
- Hernias
- Inflammatory bowel disease
- Colonic volvulus (sigmoid, cecal, transverse colon)
- Adhesions
- Constipation
- Fecal impaction
- Fecaloma
- Colon atresia
- Intestinal pseudoobstruction
- Endometriosis
- Narcotic induced, especially w/ the large doses given to cancer or palliative care Pt's
Dx
- Blood tests
- Imaging, including:
- Abdo x-ray, which may show bowel distension, and presence of multiple (>6) gas fluid levels on supine and erect abdominal radiographs. The appearance of water-soluble contrast in the cecum on abdo x-ray w/in 24 hours of oral administration predicts resolution of an adhesive small bowel obstruction
Source: Slideshare CDN
{kind=link}
-
- Luminal contrast studies, including contrast enema, small bowel series, or CT, can define the level of obstruction, whether the obstruction is partial or complete, and define the cause of obstruction
- U/S
- Biopsy, to determine the nature of the mass, if a mass is identified
- Colonoscopy, small bowel investigation w/ ingested camera or push endoscopy, and laparoscopy
Patient information
What can you do to look further into an obstruction in the intestine?You can start with bloods. You can also take images, including an x-ray of the tummy. Because x-rays aren't that good to see soft tissue, you can use contrast to outline the inside of the GI tract. Or you can use ultrasound or CT, which is better for soft tissue. You can also put a camera down the throat, to look inside, and pinch a bit of the thing that's causing the blockage.
DDx
- Ileus
- Pseudo-obstruction or Ogilvie's syndrome
- Intra-abdominal sepsis
- Pneumonia, or other systemic illness
Tx
- Mostly Tx conservatively over 2-5 days (e.g. in Crohn's disease, peritoneal carcinomatosis, sclerosing peritonitis, radiation enteritis, and postpartum bowel obstruction), because in many cases, the bowel will open up. Some adhesions loosen up, and the obstruction resolves. However, this requires close monitoring, examined several times a day, and x-rays taken to ensure the Pt is not clinically getting worse. It includes:
- Insertion of an NG tube, to correct dehydration and electrolyte abnormalities
- Opioid pain drugs, can be used for Pt's w/ severe pain
- Antiemetics, if the Pt is vomiting
- Surgical intervention to Tx the causative lesion, in surgical emergencies (e.g. volvulus, closed-loop obstructions, ischemic bowel, incarcerated hernias, fully lodged foreign object, malignant tumor), including bowel resection or lysis of adhesions
- Endoscopically placed self-expanding metal stents, may be used to temproarily relieve the obstruction as a bridge to surgery, or as palliation, in malignant large bowel obstruction
- NG tube inserted from the nose into the stomach, to help decompress the dilated bowel. The tube is uncomfortable but does relieve the abdominal cramps, distension and vomiting
- IV therapy
- Catheter in the bladder, to monitor urine output
Patient information
What can you do about an obstruction in the intestine?If the patient isn't eating, you can put a tube down their nose and feed them that way. If they're in pain or vomiting, you can also fix that. You can do open surgery. Or you may be able to use a stent to relieve any obstruction that you find.
Complications
- Dehydration
- Electrolyte abnormalities, due to vomting
- Respiratory compromise, from pressure on the diaphragm by a distended abdomen, or aspiration of vomitus
- Bowel ischemia or perforation from prolonged distension or pressure from a foreign body
Patient information
What are the things you're worried about, in an obstruction in the intestines?All the vomiting can cause a patient to become dehydrated, and affect electrolytes. The expanding mass in the tummy, can also put pressure on the diaphragm, even affecting the patient's breathing. A blockage can also cause the tummy system to blow up, or put pressure against it's blood supply, and kill parts of it.
Prognosis
- It is a medical emergency
- Some causes of bowel obstruction may resolve spontaneously
- 6% of small bowel obstruction, are ultimately fatal if Tx is delayed
See also
- Abdominal examination
Synonyms:
Intestinal obstruction
Large bowel obstruction
Large intestinal obstruction
Large intestine obstruction
Obstruct
Obstructing
Obstruction
SBO
Small bowel obstruction
Small intestinal obstruction
Small intestine obstruction
Find a practitioner
Amanda Gordon
Female PsychologistArmchair Psychology - Edgecliff NSW
Practitioner count: 0
Sponsor a disease. And see how your proceeds help.
$1
Express interest
$10
Write text
$40
Write FAQ
$100
Snap photos
$400
Record audio
$1k
Produce video
$4k
Interview experts