Definition of "Heart attack"
Heart attack (aka myocardial infarction) is where blood [and thus oxygen] flow stops to a part of the heart, and heart muscle becomes damaged.
Patient information
What is a myocardial infarction, and how does it relate to a heart attack?They mean the same thing. Infarct means tissue dies because it's blood's supply is interrupted. Myocardium is the muscle tissue of the heart, that contracts to push blood out of the heart. So MI=heart attack.
So what does heart attack exactly mean?
Death of heart muscle, because it's blood supply is interrupted.
- Causes include:
- Complete blockage of a coronary artery caused by a rupture of an atherosclerotic plaque, most commonly
- Coronary artery spasm, which may be due to cocaine, significant emotional stress (Takotsubo cardiomyopathy), extreme cold
Sx of acute MI includes:
- Sudden chest pain or discomfort, felt behind the sternum or L of the chest, and sometimes travels to the LHS arm, LHS neck, shoulder, back or jaw. It lasts for more than few minutes. The discomfort may occasionally feel like heartburn. NB: Up to 64% of Pt's, especially women, do NOT experience chest pain, and is known as silent MI
- SOB
- Diaphoresis (cold sweat)
- Nausea, vomiting
- Palpitations
- Anxiety
- Weakness, fatigue (feeling tired)
- Presyncope (feeling faint)
Patient information
What happens in a heart attack?Sudden chest pain, which is felt behind the breastbone where the heart is. It sometimes travel to the left arm or neck. You also feel short of breath.
For CAD and MI:
- Previous cardiovascular disease
- Old age
- Tobacco smoking
- Hyperlipidemia
- Diabetes
- HTN
- Lack of physical activity, obesity
- Chronic kidney disease
- Poor diet
- Excessive alcohol consumption
- Use of cocaine and amphetamines
- Family Hx of cardiovascular disease
- More common in men
Patient information
What makes it more likely for you to get a heart attack?If you've got other heart problems. Old age. Smoking. Lots of fat in your blood. Diabetes. High blood pressure. Being overweight. Not exercising. Problems with your kidney. Excessive alcohol intake. Use of recreational drugs. Other people in your family with heart problems. Being male.
- According to thickness:
- Transmural AMI (full thickness), is associated w/ atherosclerosis involving a MAJOR coronarya artery. It extends through the whole thickness of the heart muscle, and are usually a result of COMPLETE occlusion of the area's blood supply. It is evidenced on ECG by ST elevation, and Q waves. It includes:
- Anterior
- Posterior
- Inferior
- Lateral
- Septal
- Subendocardial AMI (partial thickness), involving a small area in the subendocardial wall of the L ventricle, ventricular septum, or papillary muscles. The subendocardial area is particularly susceptible to ischemia. It is evidenced on ECG by ST depression, and T wave changes
- Transmural AMI (full thickness), is associated w/ atherosclerosis involving a MAJOR coronarya artery. It extends through the whole thickness of the heart muscle, and are usually a result of COMPLETE occlusion of the area's blood supply. It is evidenced on ECG by ST elevation, and Q waves. It includes:
- According to the appearance of an ECG:
- For STEMI (ST elevation MI, i.e. where the ST traces higher than baseline) (30%), which presents with ST elevation, pathological Q waves, is a transmural infarction (i.e. full thickness of heart muscle), resulting in complete occlusion of the area's blood supply. It is associated with CAD
- For non-STEMI (non-ST elevation MI) (25%), which presents with ST depression, is a subendocardial MI
Patient information
What are the types of myocardium death?STEMI, and non-STEMI. STEMI means that on the ECG, there is ST elevation, and pathological Q waves. And non-STEMI where there isn't ST elevation, but rather, depression.
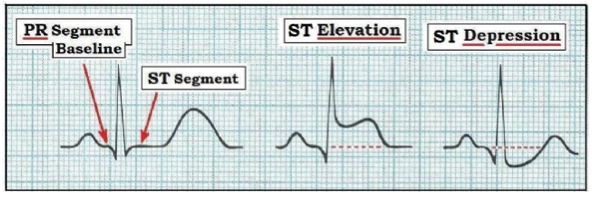
What's this ST elevation or depression about? What is ST?
ST should be flat. ST is the point between depolarization (QRS wave) and repolarization (T-wave) of the ventricles. So it should be flat. But if heart muscle is damaged, it's contractile and electrical properties change. This causes early repolarization, prematurely ending the pumping of the ventricle, called systole.
Early repolarization explains why the full-thickness ST elevation happens. But why does ST depression happen?
Where the the death of heart muscle is not full thickness, there is an elevated resting potential in heart cells. That makes the ST look like it's going down.
For CAD and MI:
- For CAD only (and not suspected MI), cardiac stress testing
- ECG's, looking for:
- ST elevation (STEMI), which usually requires more aggresive Tx
- Pathological Q waves
- ST depression, in non-STEMI, alternatively
Source: Blogspot
{kind=link}
- Blood tests, for cardiac markers, including:
- Troponin
- Creatinine kinase (CK-MB), which has since been largely replaced by troponin
- Coronary angiography, which is an x-ray with radiocontrast, in the coronary arteries
Patient information
How do you confirm a heart attack?Using an ECG, to see if there are any changes indicating heart damage. If there's nothing that can be seen, the patient can be challenged to exercise, whilst an ECG is being performed, to see if anything happens under exertion. You can also do an x-ray whilst contrast is being used to outline the arteries supplying the heart.
Any blood tests you can do?
Yeah, troponin and creatinine kinase. Troponin is released by heart muscle into blood, when it is damaged. Creatinine kinase is also released by heart muscles into blood, when it is damaged, although troponin is a better measure for this.
For CAD and MI:
- For pain:
- GTN (nitroglycerin)
- Opioids
- Oxygen, in patients with low oxygen levels or SOB
- In STEMI, restoring blood flow to the heart, using:
- Reperfusion therapy (i.e. restoring circulation to the heart), using angioplasty (aka percutaneous coronary intervention, i.e. arteries are pushed open)
- Thrombolysis (i.e. blockage removed using medications)
- In non-STEMI, using:
- Heparin (blood thinner)
- Angioplasty, in those at high risk
- CABG (coronary artery bypass surgery), for Pt's with MULTIPLE blockages of the coronary arteries, particularly if they also have diabetes
- Address risk factors, after the MI, with:
- Lifestyle modification (healthy diet)
- Aspirin, preventing further blood clots, including in a suspected MI
- Address diabetes
- Address hypercholesterolemia, with statins
- Address HTN, with beta blockers
Patient information
What can be done about a heart attack?Thrombolysis drugs, can be used to remove blockages. Because heart muscle is damaged, an antiplatelet like aspirin can be given to prevent blood clots. GTN can also be given, which produces nitric oxide, which enlarges the blood vessels. The only problem with GTN is it can only be used in the short term, as it will result in tolerance after 2-3 weeks of use. You can also do things like address risk factors, including a healthy diet, address diabetes, high cholesterol, and high blood pressure.
Any surgery you can do?
Angioplasty, and CABG. Angioplasty is where a balloon is used to widen narrowed or obstructed arteries. CABG is where a vessel is used to divert blood flow away from an obstructed artery supplying the heart.
For Prinzmetal angina:
- Atropine
Patient information
Anything you can do for chest pain caused by spasm in the arteries supplying the heart?Atropine. It's an anticholinergic, so it inhibits the parasympathetics. This therefore causes dilation of the blood vessels.
- Acute complications, include:
- Heart failure, if the damaged heart is no longer able to pump blood adequately around the body
- Cardiac arrest
- Aneurysm of the LV myocardium
- Ventricular septal rupture, or free wall rupture
- Mitral regurgitation, in particular if the infarction causes dysfunction of the papillary muscle
- Dressler's syndrome
- Abnormal heart rhythms, e.g. ventricular fibrillation
- Ventricular tachycardia
- Atrial fibrillation
- Heart block
- Long term complications, including:
- Heart failure
- Atrial fibrillation
- Increased risk of a second MI
Patient information
What can death of heart muscle cause?The failure of the heart to work.
- Worldwide >3m people have STEMI's, and 4m have NSTEMI's
- STEMI occurs about twice as often in men as women
- In the developed world, the risk of death in those who have STEMI is about 10%
- Rates of MI for any given age have decreased globally between 1990 and 2010
- Leading cause of death in the world
- In those >75yo, 5% have had an MI with little or no Hx of Sx
- Acute coronary syndrome (category)
- Unstable angina (cardiac markers are negative, cf positive cardiac markers in MI)
- Coronary artery disease/ischemic heart disease
- CABG (Tx)
- Angioplasty (Tx)
Find a practitioner
Practitioner count: 0